Ceramics in dentistry
Ceramics for dental restorations have evolved from fragile materials made from naturally-occurring minerals to high-strength synthetic ceramics of today. Manufacturing techniques have moved from purely manual processing to computer assisted design and manufacture (CAD/CAM). The development has been rapid during the last 20 years and is still ongoing regarding the balance of esthetics and strength, and cementation procedures.
The present theme present elements of properties, applications and clinical performance of contemporary dental ceramics.
Ceramic materials and their different applications have become an essential part of contemporary restorative and prosthetic dentistry. The tooth-like appearance of ceramic materials has made them desirable for replacing and restoring dental hard tissues dating back to 18th century. In the last decades there has been a formidable development in both materials and processing techniques (Figure 1). The three main issues in the development of dental ceramics have been to improve the dimensional accuracy of ceramic restorations, increase flexural strength, and to make the appearance more natural-looking
Dental ceramics of today constitute a heterogeneous group of materials with significant differences in mechanical and optical properties as well the ability to be bonded to teeth with resin-based cements. A favorable clinical outcome depends on material selection, manufacturing technique, restoration design, and compliance with recommended procedures. The dental practitioner therefore needs good knowledge about the indications, limitations, and correct use of materials. Moreover, computerized design- and manufacturing technologies (CAD/CAM) at the dental laboratories have expanded the applications of ceramics (1).
The present theme aims to provide evidence-based information on the properties, indications and contraindications, and clinical outcomes with regard to contemporary dental ceramics. Also, examples are provided to show clinical applications in young people and in other challenging situations.
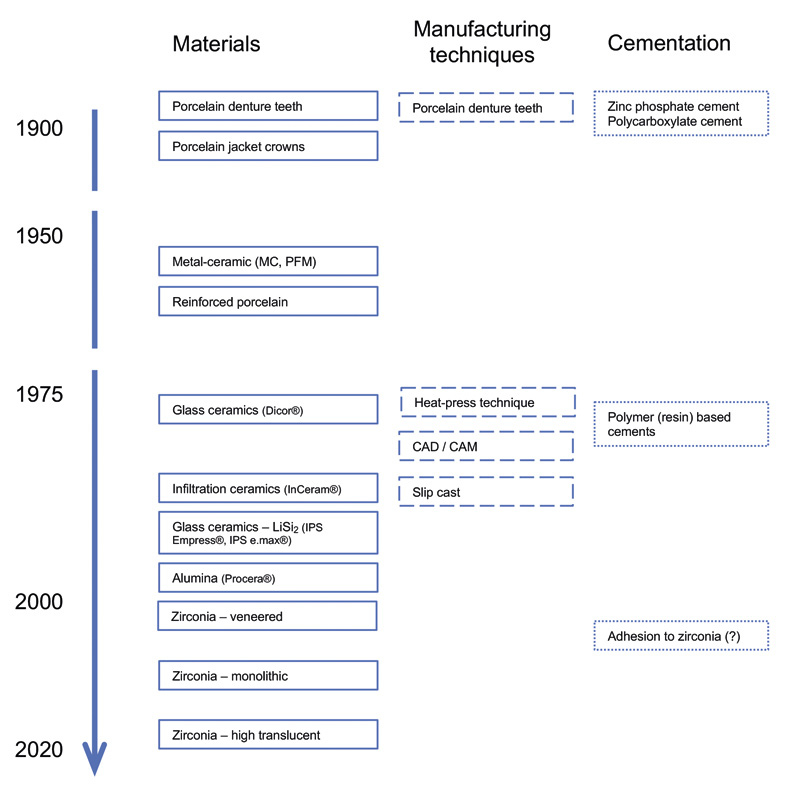
Figure 1. Timeline of the evolution of ceramic restorative materials.
Properties of ceramics
Ceramic materials are inorganic, non-metallic, solid materials comprising metal, non-metal or metalloid atoms forming a ceramic structure in combination with oxygen for instance (2). The ceramic materials constitute atoms with ionic or covalent bonds, and can be crystalline, amorphous or comprise a combination (3). The restorative materials are usually chemically stable, strong and hard but are susceptible to brittle fracture, in contrast to metals and alloys, which exhibit plastic deformation when overloaded. Moreover, pores and other microstructural flaws or cracks present in the material can create stress concentrations, when - if the shape and size of the flaw is critical - will cause failures. Thus, resistance to crack growth is fundamental to make a strong and tough ceramic. A typical clinical failure mode for a ceramic restorations with low to moderate toughness, for example feltspatic ceramic, is total fracture, whereas materials with high toughness, for instance stabilized zirconium-dioxide (zirconia), show failure modes more similar to that of metals.
Mechanical properties - common terms
Mechanical data are frequently used in presentations and in promotional material to describe the properties of different ceramics. There are numerous test procedures that can be applied. The present international standard (4) uses flexural strength as the main physical characteristic of the different classes of dental ceramics. However, more refined test methods could be included in future standards, for example fatigue testing.
Ultimate strength - is a material's maximum ability to resist mechanical stress before it fails. Typically, strength of ceramics is measured by a flexural test, by supporting a beam (bar) at each end, and loading it in either a three point or four-point bending test. During testing the test beam is under compressive stress at the concave surface and tensile stress at the convex surface (3, 5, 6). Ceramics tend to fail under tensile stresses.
Fracture toughness - describes the material's ability to resist fracture as a consequence of the ever-present submicroscopic flaws. A high toughness indicates high damage tolerance which in practice means being less brittle. Fracture toughness is often described by the critical stress intensity factor (KIc), which is a measure of the stress concentration at the tip of an existing flaw (3, 7).
Modulus of elasticity - is a material property that describes the relative deformation - strain - related to the applied stress, expressed as the ratio of stress to strain. Materials with a high modulus of elasticity are stiff, like most ceramics, whereas those with a low modulus are flexible, typically polymers (3, 6).
Dental ceramics - terminology and classification
The terminology concerning dental ceramics might be confusing. The term monolithic is used for restorations that are substantially made of a single uniform material. This is also called full contour in some contexts. The layered restorations are made with a core covered by another type ceramic, for example a zirconia core with feltspatic veneer.
Contemporary dental ceramic materials can be classified into three subgroups (Table 1): Predominantly glassy materials, usually termed feltspatic ceramics or just porcelains. Then there are particle-filled glasses, also known as glass-ceramics, and, finally, polycrystalline ceramics, also known as oxide ceramics (8-10). Materials in this subgroup differ in terms of both bonding properties and strength. Stronger ceramics tend to be more challenging to bond to tooth structures.
The current ISO standard (4) presents a classification based on applications. Class 1 ceramics are designed for veneering of metal or high-strength core ceramics. Bonding to teeth are easily achieved. Class 5 ceramics, at the other end of the scale, constitute materials designed to withstand the stresses in prostheses with four units or more.
Variations |
Aesthetics |
Strength, mechanical properties |
Processing technique |
Clinical use |
|
|---|---|---|---|---|---|
Variations |
Aesthetics |
Strength, mechanical properties |
Processing technique |
Clinical use |
|
Porcelains.Feldspatic ceramic |
Crown materials. Veneering materials |
+++ |
- |
Slurry technique (hand application), pressing, milling |
Veneers. bonded monolithic crowns |
Glass-ceramic |
Glass-ceramics, lithium disilicates (LiSi2), combinations with zirconia |
+ - +++ |
+ - ++ |
Pressing, casting, milling |
Veneers, bonded monolithic crowns, bi-layer restorations, anterior short bridges |
Polycrystalline ceramic.Oxide ceramic |
Alumina (obsolete) |
+ |
++ |
Predominantly milling |
Frameworks for bi-layered restorations, monolithic restorations, bridges, resin-bonded cantilever bridges |
Zirconia, ultra-translucent (anterior) |
++ |
++ |
|||
Zirconia, translucent (posterior) |
+ |
+++ |
|||
Zirconia, for cores (frameworks) |
- |
+++ |
Feltspatic ceramics. Porcelains
These materials are traditionally termed porcelains, although that is not accurate from a material science viewpoint. The restorations can be created from powders applied in layers by hand. These predominantly glassy materials are not strong enough to withstand occlusal forces without support from a metal- or a high-strength ceramic core. They are mainly used as veneering materials but can additionally be used as monolithic porcelain laminate veneers where the tooth itself supports the ceramic. The high glass content of traditional porcelains makes them good substrates for resin bonding through silane coupling agents. This feature also makes it possible to repair veneering ceramic fractures intraorally.
Glass ceramics
Glass ceramics are crystallized glasses where the strengthening crystallization is achieved by a controlled heat treatment of the restoration. Examples of dental glass ceramics are leucite-based or lithium-disilicate based ceramics that provide adequate mechanical properties, easy bonding to tooth structures using polymer (resin) cements. Glass ceramics are commonly used to make monolithic restorations, but can also be combined with porcelain veneers. Their optical properties are attractive for restorations where the esthetic demand is high. They are successfully used for indirect adhesive restorations and crowns in both anterior and posterior teeth.
Polycrystalline ceramics (oxide ceramics)
Polycrystalline oxide ceramics, such as zirconia and alumina, are the strongest and toughest dental ceramics. The good mechanical properties of stabilized zirconia enable its use even in long-span bridges in the posterior area (11). However, the polycrystalline material lacks a glass phase and cannot be easily etched with traditional methods. Therefore the adhesion is based on mechanical retention and a chemical bond between zirconia and for example adhesives containing 10-methacryloxydecyl-dihydrogenphosfate (MDP). Good clinical outcomes can be achieved even in high-stress restorations (12). This is presently a field of high research interest.
In clinical studies of zirconia restorations, the most common complication seems to be chipping of the veneering ceramic (13). Hence, the use of zirconia has moved from fully veneered porcelain-fused-to-zirconia structures into monolithic (full contour) zirconia structures. Recently, so-called ultra or high translucent zirconia materials have been introduced to improve the optical properties of monolithic restorations. However, the improvement in cosmetic features seem to be achieved at the cost of mechanical properties. Long-term clinical data are highly desired.
The editorial committee hopes that the papers of the theme will cast light on the complex and rapidly evolving ceramic materials and technologies made available to dental practitioners.
The editorial committee
Nils Roar Gjerdet (coordinator, the Norwegian Dental Journal), Klaus Gotfredsen (Copenhagen), Johanna Tanner (Åbo/Turku), Per Vult von Steyern (Malmö), and Marit Øilo (Bergen).
References
Vult von Steyern P, Ekstrand K, Svanborg P, Örtop A. Framställning av protetiska konstruktioner med hjälp av moderna digitala teknologier - en översikt. Tandlakartidn. 2014; 106(2): 56-66.
Vult von Steyern P. Dental Ceramics in Clinical Practice. In: Nilner K, Karlsson S, Dahl BL, editors. A Texbook of Fixed Prosthodontics The Scandinavian Approach. 2nd ed: Förlagshuset Gothia AB; 2013. p. 205-22.
O'Brian. Dental Materials and Their Selection. 4th ed: Quitessence Publishing Co, Inc.; 2008.
ISO. Dentistry - Ceramic materials. ISO 6872. Geneva, Switzerland: ISO; 2015.
Ashby MF. Materials Selection in Mechanical Design. 4th ed: Elsevier B.V.; 2011.
Darvel BW. Materials Science for Dentistry. 10th ed: Woodhead Publishing Series in Biomaterials; 2018.
Cesar PF, Della Bona A, Scherrer SS, Tholey M, van Noort R, Vichi A, et al. ADM guidance-Ceramics: Fracture toughness testing and method selection. Dent Mater. 2017; 33(6): 575-84.
Giordano R, 2nd. A comparison of all-ceramic restorative systems: Part 2. Gen Dent. 2000; 48(1): 38-40, 3-5.
Kelly JR. Ceramics in restorative and prosthetic dentistry. Annu Rev Mater Sci. 1997; 27: 443-68.
Kelly JR, Benetti P. Ceramic materials in dentistry: historical evolution and current practice. Aust Dent J. 2011; 56 Suppl 1: 84-96.
Denry I, Kelly JR. State of the art of zirconia for dental applications. Dent Mater. 2008; 24(3): 299-307.
Kern M, Passia N, Sasse M, Yazigi C. Ten-year outcome of zirconia ceramic cantilever resin-bonded fixed dental prostheses and the influence of the reasons for missing incisors. J Dent. 2017; 65: 51-5.
Pjetursson BE, Sailer I, Makarov NA, Zwahlen M, Thoma DS. All-ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part II: Multiple-unit FDPs. Dent Mater. 2015; 31(6): 624-39.
Artikkelen er fagfellevurdert.
Artikkelen siteres som:
Gjerdet NR, Gotfredsen K, Tanner J, Vult von Steyern P, Øilo M. Ceramics in dentistry. Nor Tannlegeforen Tid. 2019;130:08-11. doi:10.56373/2019-1-3