
The role of the dental team in domestic abuse cases
Clinical relevance box
Injuries from abuse are often located in the head, neck, and oral region – areas routinely examined by dental professionals.
A forensic approach in dental practice enhances the early detection and documentation of non-accidental injuries.
Dental teams must be aware of injury patterns, behavioral signs, and vulnerability factors associated with abuse and neglect.
Clear guidelines and training are essential to support dental professionals in fulfilling their legal and ethical duty to report suspected abuse.
Collaboration with forensic odontologists can strengthen the quality of injury documentation and support legal processes.
Abbreviations used in the text
DV Domestic Violence
IPV Intimate Partner Violence
CC Coercive Control
CAN Child Abuse and Neglect
ACEs Adverse Childhood Experiences
HNF Head, Neck, and Face
STIs Sexually Transmitted Infections
OHQoL Oral Health-Related Quality of Life
FDV Family and Domestic Violence
Domestic violence is a prevalent public health issue that primarily affects women and children. Its impact on oral health includes head, neck, and facial injuries, irregular dental visits, and dental fear, making dental professionals well-positioned to identify signs of abuse in clinical settings. However, uncertainty, lack of training, and concerns about patient confidentiality often lead to missed recognition and inaction. In the Nordic countries, dental professionals have both a legal and ethical duty to report suspected DV, and in Sweden, public-sector dentists are required to provide forensic injury reports upon request from law enforcement.
This overview highlights how individuals affected by various forms of DV can be identified in dental settings, with a focus on recognizing traumatic injury patterns, dental diseases, and behavioural indicators for early detection. It also emphasizes the importance of accurate documentation when suspicion arises. Forensic odontologists play a crucial role in supporting dental teams through expert consultation, education, and training. Integrating forensic awareness into routine dental practice strengthens the ability to detect, document, and report suspected abuse – facilitating early intervention and contributing to justice for vulnerable individuals.
Domestic violence, including intimate partner violence, refers to a persistent pattern of physical, sexual, or psychological harm within close relationships. A central component is coercive control – a systematic use of manipulation, intimidation, and domination intended to instill fear and maintain power over the victim [1]. This control is often exerted through physical aggression, sexual coercion, psychological abuse, and other controlling behaviors [2].
DV also encompasses other forms of abuse occurring within domestic settings, such as child abuse and neglect, elderly abuse, or violence between siblings. Despite being extensively researched and recognized as a political priority, DV remains a widespread societal and public health concern [3]. Although both men and women can be victimized, IPV is generally acknowledged as a gendered form of violence, predominantly affecting women, both in terms of frequency and severity of injuries sustained [4]. Epidemiological data suggest that approximately one in three women has experienced IPV at some point in her lifetime [5].
The well-documented negative health consequences of DV affect survivors both in the short and long term, encompassing psychological conditions such as anxiety and depression, physical injuries, and, in some cases, fatal outcomes [6]. Child abuse and neglect take many forms and have long-lasting effects on a child’s emotional and physical well-being, including oral health. Traumatic life experiences, including adverse childhood experiences (ACEs), such as physical, sexual, or psychological abuse, neglect, bullying (including online), and other forms of exploitation, can have lasting adverse effects on the individual’s functioning and physical, social, emotional, or spiritual well-being [7][8].
Research also shows that exposure to violence during childhood can have profound effects on health trajectories, including oral health. For instance, a Norwegian study reported that children suspected of sexual abuse had four times more caries and restorations in permanent teeth compared to those suspected of physical abuse [9]. Additional data from the Young-HUNT Survey in Norway [10] (n = 6,526; ages 13–19) revealed that 42,4% of adolescents had experienced at least one adverse childhood experience, including physical abuse, witnessing violence, and sexual abuse [11]. These findings underscore the long-term and multisystemic impact of domestic violence, particularly among vulnerable groups such as children and adolescents.
The aim of this review is to describe various forms of DV, their manifestations, and the role of dental professionals in identifying, documenting, and reporting abuse, emphasizing the importance of integrating forensic awareness into routine dental examinations for early detection and intervention.
Recognizing domestic violence in the dental clinic
Detecting DV in dental settings requires attention to both patient behavior and clinical signs. While physical injuries may not always be present, other indicators can suggest abuse. Financial abuse, for example, may prevent patients – particularly women – from affording or accessing dental care. Controlling behaviors, such as withholding child support or restricting healthcare decisions, can lead to delayed or missed appointments [12]. Additionally, signs such as dental fear and anxiety may be indicative of trauma. Women with a history of sexual abuse often describe dental care as triggering, leading to avoidance behaviors, disruptions in daily routines, and a decline in oral hygiene practices, including reduced tooth brushing and a reluctance to attend to dental appointment [13][14].
Risk factors of domestic violence
Identifying individuals at risk of DV in dental practice is challenging. Warning signs may include unexplained injuries, evasive behavior, or the presence of a controlling partner during appointments. The patient’s broader social context also matters. For instance, children who live in violent households are at heightened risk of physical abuse, and in Sweden, simply residing in such an environment constitutes a criminal offense [15].
Risk factors span multiple levels of the socio-ecological model [16]. Individual-level factors include prior abuse, financial dependence, and traditional gender roles. At the relationship level, unequal power dynamics, controlling behavior, and economic disparities increase vulnerability [17]. Dental professionals should also recognize vulnerability factors that heighten the risk of domestic violence, such as low socioeconomic status, mental illness, substance abuse, a history of trauma, or chronic illness – each of which can hinder an individual’s ability to seek help or self-protect [18][19].
Injury characteristics in domestic violence
Understanding injury patterns and assessing the trauma history as told by the patient is crucial for identifying and addressing abuse across various populations. Oral injuries in both children and adults subjected to abuse commonly result from direct physical violence to the face, such as punching or slapping, which can cause dental trauma, mucosal lacerations, and jaw fractures. Additional mechanisms include forced feeding, gagging, rubbing, biting and strangulation which may lead to soft tissue injuries in the lips, gums, oral mucosa and throat [20][21] (table 1). The spectrum of abusive injuries ranges from discrete, barely recognizable, impacts to fatality [22][23].
In victims of physical abuse, bruises are the predominant injury type (e.g. 1) appearing with a reported prevalence of around 70% among abused children [22] and 26–57% in adults and elderly [17][24]. Other abuse-related injury types include soft tissue lacerations, fractures and internal injuries [4]. Danish data from a forensic cohort of children (0–18 years) referred for suspected physical abuse showed skin lesions in 72% (head), 70% (arms/hands), 60% (trunk), 37% (legs/feet), 31% (neck), and 17% (genital/buttock region), with bruises accounting for nearly 50% of lesions. Over 40% of children under two had occult fractures, underscoring the need for full-body X-rays in suspected cases [23].
Among women exposed to DV, injuries of the head, neck and face (HNF), including the oral cavity, are highly prevalent, with studies showing that 13–75% of abuse victims sustain trauma to these areas [4][25]. The prevalence rates and clinical finding of injuries associated with HNF/Dental varies significantly based on the study population and data collection methods. A Portuguese study analyzing 332 forensic reports found that 13,4% of IPV cases involved oral injuries [26]. These injuries predominantly affected soft tissues, including the lips, oral mucosa, and tongue. A more recent review by Souza Cantão et al. [27] revealed that 29% of women exposed to FDV had oral and facial injuries, while 4% suffered from dental trauma.
Differentiating between accidental versus non-accidental injuries
Since traumatic injuries alone rarely prompt dental practitioners to suspect violence, the key lies in distinguishing accidental from inflicted injuries. In dependent individuals, such as children or those with disabilities, accidents may signal neglect due to inadequate supervision. Recent efforts have aimed to identify injury patterns that support early suspicion and forensic assessment. Accidental injuries in children typically occur on bony prominences – such as the forehead, knees, and elbows – and align with the child's developmental stage. In contrast, non-accidental injuries are often located in protected areas – such as the ears, neck, and inner arms – and may exhibit recognizable patterns (e.g., handprints, bite marks) or occur at varying stages of healing. Delayed care-seeking, inconsistent caregiver explanations, and behavioral changes further raise suspicion [28].
Tools like the TEN-4 rule (bruising on torso, ears, neck, or any bruising in infants <4 months) has proven useful in distinguishing abuse from accidental injury [29]. Cairns et al. [30] highlighted that most physically abused children present injuries easily visible during dental exams, especially in the «triangle of safety» (ears, side of face, neck, and shoulders), where accidental injuries are rare [28] (figure 1).
Dental professionals, who routinely examine the face under strong lighting, are well-positioned to detect these injuries if properly trained [31][32]. In adults, facial trauma resulting from interpersonal violence is often associated with a higher incidence of facial bone fractures and skin lacerations. Conversely, accidental injuries more frequently affect prominent areas of the face and neurocranium [33].
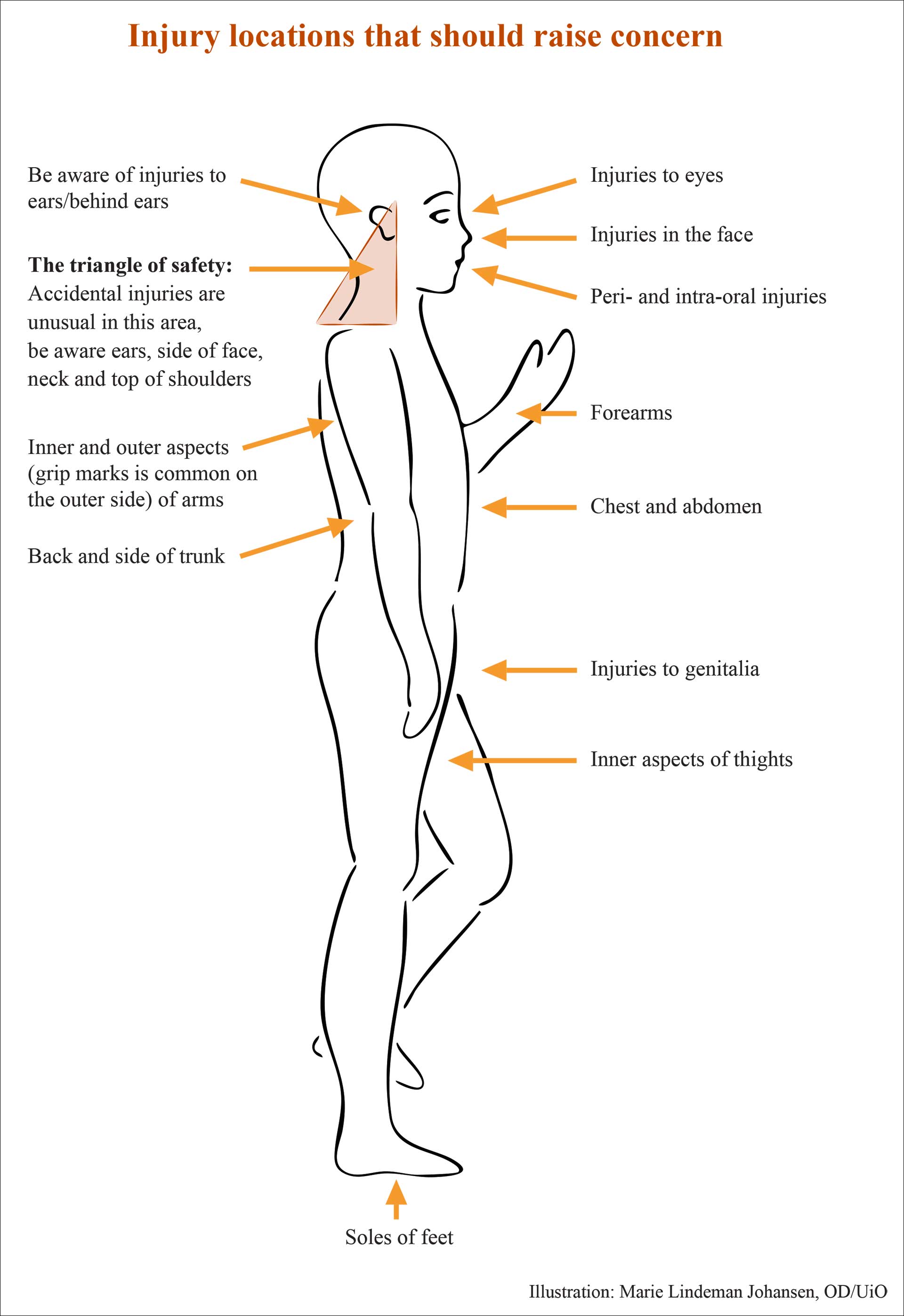
Figure 1. Typical injury locations in accidental versus non-accidental trauma.
Dental neglect
Dental neglect occurs when a caregiver fails to provide and comply with adequate dental care, leading to dental pain, infection, or significant deterioration of a child's or dependent individual's oral health [12]. Also applicable among adults and elderly in need of assistance. It is recognized as a serious but often overlooked subset of medical neglect that can have significant consequences for a child's overall health and well-being [21]. Furthermore, dental neglect is often associated with broader patterns of social vulnerability and various forms of abuse [34][35]. According to a review of 147 reports from the dental profession to the social services, the primary cause of reporting was parental deficiencies in care, followed by a concern of dental neglect [35][36]. Lack of parental engagement may be identified through repeated missed and cancelled appointments despite urgent dental needs and/or seeking necessary treatment [21]. Key indicators include untreated caries and, often leading to pain, infections, abscesses, or difficulty eating [37]. Poor oral hygiene and periodontal disease with clinical observable thick plaque and calculus buildup, gingivitis, or severe periodontal disease where the caregiver consistently fails to adhere to recommendations. ACEs have also been linked to poor oral health outcomes, including associations with inadequate oral hygiene habits, increased caries prevalence, and missed dental appointments [11]. Affected children may experience anxiety, shame, and fear of losing control, which can contribute to dental anxiety and reduced oral health-related quality of life [38].
The role of the dental profession in detecting and reporting DV
Dental professionals must be alert to signs of violence in both children and adults and are uniquely positioned to identify, intervene, and protect individuals at risk, for example by [19][21][39][40]:
Seeing patients regularly, which allows for ongoing monitoring and trust-building that may reveal mistreatment.
Working in well-lit environments with clear visibility of the head and neck area.
Being trained to recognize signs of abuse, which may appear as facial injuries, oral trauma, or dental neglect.
Noticing behavioral changes, such as missed appointments, that may indicate abuse or neglect.
In the Nordic countries, dental and healthcare professionals are legally and ethically required to report suspected child abuse or neglect to child welfare services without exception [19]. Reporting is mandatory, and if a criminal offence or evidence tampering is suspected, the police should also be notified. The same duty applies in cases of domestic violence to protect patient safety [39][41][42]. Despite this duty, underreporting by dental professionals remains common in the Nordic countries and beyond [42][43][44][45][46]. A recent Norwegian study, however, shows increased reporting among general dentists [43].
Research indicates that healthcare professionals who often treat patients affected by DV, rarely conduct routine screenings, even when managing injuries related to abuse [47][48][49]. There are several reasons for reluctance to report, including uncertainty, lack of guidelines, and limited knowledge of referral procedures [43][44][50][51] (table 2). Emotional concerns may arise when the suspected perpetrator is known to the dental team, potentially affecting trust. However, the duty to report suspected abuse takes precedence over patient confidentiality [43][44]. Reporting a suspicion of neglect, abuse and violence is always with the individual´s best interest in mind.
Documentation
Dental records are a critical source of information in suspected cases of domestic violence. Patient-reported trauma history, reasons for dental fear, and financial difficulties may indicate an abusive context and should be carefully documented. Social, medical, and dental history, along with any suspicion of maltreatment, must be recorded thoroughly. In children, documentation should include dialogue with caregivers regarding dental caries, treatment plans, and their adherence to recommendations. Attendance records, cancellations, and reasons for missed appointments may also support child welfare investigations. For trauma cases, both extraoral and intraoral findings should be described in detail, alongside any behavioral observations. Accurate written descriptions on injuries, clinical photographs, and radiographs are essential [19][21][28]. All reports of suspected abuse must be clearly and securely documented, including the rationale for reporting. Patients – and guardians – have the right to access their records [19]. Most Nordic electronic record systems now offer options to safeguard DV-related information using protected keywords accessible only to authorized personnel.
Forensic aspects in dentistry and abuse cases
A forensic approach in general dentistry is crucial for accurately documenting injuries that may serve as legal evidence. However, most dental professionals receive limited training in recognizing abuse-related oromaxillofacial injuries, distinguishing them from accidental trauma, and meet forensic documentation standards. Unlike routine records, forensic documentation requires detailed injury descriptions, high-quality clinical photographs with scale, and radiographs to detect hidden trauma.
Forensic odontologists serve as a link between dentistry and law enforcement, providing expert guidance in injury assessment, report writing, and legal proceedings. In Sweden, public-sector dentists are legally required to issue forensic certificates upon request from law enforcement, yet many lack clarity on how to fulfill this duty. Involving forensic odontologists in dental education through specialized training can strengthen dental teams’ competence, preparedness, and confidence in managing suspected abuse cases.
Conclusions
Dental professionals play a crucial role in detecting domestic violence, as many abuse-related injuries involve the head, neck, and oral region – areas routinely examined in dental care.
Underreporting remains a major issue, often due to uncertainty, lack of forensic training, and fear of breaching confidentiality. Strengthening knowledge and clear reporting guidelines is essential for improving response.
Thorough and objective documentation is critical for patient safety, legal proceedings, and safeguarding vulnerable individuals. A forensic approach should be integrated into everyday dental practice.
Forensic odontologists have a key role in supporting the dental profession through education, expert guidance, and collaboration with legal authorities. Their involvement enhances both the quality of documentation and the likelihood of appropriate intervention.
References
Stark E. Coercive control: The entrapment of women in personal life. New York: Oxford University Press; 2009.
World Health Organization. Violence against women. 2024. [Internett]. Tilgjengelig fra: https://www.who.int/news-room/fact-sheets/detail/violence-against-women
Coulthard P, Yong SL, Adamson L, Warburton A, Worthington HV, Esposito M, et al. Domestic violence screening and intervention programs for adults with dental or facial injury. Cochrane Database Syst Rev. 2010;8(12):CD004486. https://doi.org/10.1002/14651858.CD004486.pub3.
Amin D, Manhan AJ, Zeidan AJ, Evans DP, Abramowicz S, Smith RN. Do gender differences exist among victims of head and neck injuries due to intimate partner violence? J Oral Maxillofac Surg. 2023;81(1):49–55. https://doi.org/10.1016/j.joms.2022.10.002.
World Health Organization. Violence against women prevalence estimates, 2018: global, regional and national prevalence estimates for intimate partner violence against women and global and regional prevalence estimates for non-partner sexual violence against women. Executive summary. Geneva: World Health Organization; 2021.
Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359(9314):1331–6. https://doi.org/10.1016/S0140-6736(02)08336-8.
Bali D, Pastore M, Indrio F, Giardino I, Vural M, Pettoello-Mantovani C, et al. Bullying and cyberbullying increasing in preadolescent children. J Pediatr. 2023;261:113565. https://doi.org/10.1016/j.jpeds.2023.113565.
SAMHSA. SAMHSA's concept of trauma and guidance for a trauma-informed approach. Substance Abuse and Mental Health Services Administration. Rockville, MD: SAMHSA; 2014.
Toft J, Myhre AK, Sun Y-Q, Willumsen T, Rønneberg A. Oral health history in children referred to a child advocacy center in Norway. Child Abuse Negl. 2022;132:105789. https://doi.org/10.1016/j.chiabu.2022.105789
Åsvold BO, Langhammer A, Rehn TA, Kjelvik G, Grøntvedt TV, Sørgjerd EP, et al. Cohort profile update: the HUNT Study, Norway. Int J Epidemiol. 2023;52(1):e80–91. https://doi.org/10.1093/ije/dyac095.
Myran L, Sen A, Willumsen T, Havnen A, Kvist T, Rønneberg A, et al. Associations of adverse childhood experiences with caries and toothbrushing in adolescents: The Young-HUNT4 Survey. BMC Oral Health. 2023;23(1):760. https://doi.org/10.1186/s12903-023-03492-z.
Ridsdale L, Gilchrist F, Balmer, RC, Skelton R, Sidebotham PD, Harris JC. British Society of Paediatric Dentistry: A policy document on dental neglect in children. Int J Paediatr Dent. 2024;34(2):160–8. https://doi.org/10.1111/ipd.13120.
Fredriksen TV, Søftestad S, Kranstad V, Willumsen T. Preparing for attack and recovering from battle: Understanding child sexual abuse survivors' experiences of dental treatment. Community Dent Oral Epidemiol. 2020;48(4):317–27. https://doi.org/10.1111/cdoe.12536.
Wolf E, Priebe G. The self-perceived impact of sexual abuse on daily life and general health – an issue to consider in dental care. Dent Traumatol. 2024;40(Suppl 2):43–52. https://doi.org/10.1111/edt.12890.
Swedish Crime Victim Authority. Barnfridsbrott. Stockholm; 2022. https://referatsamling.brottsoffermyndigheten.se/referat-fran-den-1-juli-2022/vald-och-hot-i-nara-relation-riktat-mot-barn/barnfridsbrott/
Heise LL. Violence against women: an integrated, ecological framework. Violence Against Women. 1998;4(3):262–90. https://doi.org/10.1177/1077801298004003002.
Antai D. Traumatic physical health consequences of intimate partner violence against women: what is the role of community-level factors? BMC Womens Health. 2011;11:56. https://doi.org./10.1186/1472-6874-11-56.
Kildahl AN, Berggren T, Rønneberg A, Molnes CSY, Nordgarden H. A call for trauma-informed dental care for individuals with intellectual disabilities. Spec Care Dentist. 2024;44(4):1126–34. https://doi.org/10.11117/scd.12959.
Koch G, Poulsen S, Espelid I, Haubek D (red.). Pediatric dentistry: A clinical approach. Kap. 26. Chichester: Wiley-Blackwell; 2017.
Håkstad K, Fegran L, Hovden E, Köpp UMS. Orofacial signs of child or adolescent maltreatment identified by dentists and dental hygienists: A scoping review. Int J Paediatr Dent. 2024;34(3):285–301. https://doi.org/10.1111/ipd.13139.
Spiller LR. Orofacial manifestations of child maltreatment: A review. Dent Traumatol. 2024;40(Suppl 2):10–17. https://doi.org/10.1111/edt.12852.
Eg MB, Græsholt-Knudsen T, Madsen KB, Obel C, Charles AV, Ingemann-Hansen O. Distinct age-related differences among victims in cases of suspected child abuse. J Forensic Sci. 2024;69(1):252–263. https://doi: 10.1111/1556-4029.15398.
Frost L, Borreschmidt LQ, Bindslev DA. Skin lesions in 397 children referred for forensic medical examination on suspicion of physical abuse. Dan Med J. 2023;70(8):A10220657.
Wiglesworth A, Austin R, Corona M, Schneider D, Liao S, Gibbs L, et al. Bruising as a marker of physical elder abuse. J Am Geriatr Soc. 2009;57(7):1191–6. https://doi.org/10.1111/j.1532-5415.2009.02330.x
da Fonseca MA, Feigal RJ, ten Bensel RW. Dental aspects of 1248 cases of child maltreatment on file at a major county hospital. Pediatr Dent. 1992;14(3):152–7.
Caldas IM, Grams AC, Afonso A, Magalhães T. Oral injuries in victims involving intimate partner violence. Forensic Sci Int. 2012;221(1-3):102–5. https://doi.org/10.1016/j.forsciint.2012.04.010.
de Souza Cantão ABC, da Silva Lima TC, Fernandes MIAP, Nagendrababu V, Bastos JV, Levin L. Prevalence of dental, oral, and maxillofacial traumatic injuries among domestic violence victims: A systematic review and meta-analysis. Dent Traumatol. 2024;40(Suppl 2):33–42. https://doi.org/10.1111/edt.12922.
Harris J, Sidebotham P, Welbury R. Child protection and the dental team: An introduction to safeguarding children in dental practice. Committee of Postgraduate Dental Deans and Directors UK; 2006.
Pierce MC, Kaczor K, Lorenz DJ, Bertocci G, Fingarson AK, Makoroff K, et al. Validation of a clinical decision rule to predict abuse in young children based on bruising characteristics. JAMA Netw Open. 2021;4(4):e215832. https://doi.org/10.1001/jamanetworkopen.2021.5832.
Cairns AM, Mok JYQ, Welbury RR. Injuries to the head, face, mouth and neck in physically abused children in a community setting. Int J Paediatr Dent. 2005;15(5):310–8. https://doi.org/10.1111/j.1365-263X.2005.00661.x.
Alapulli H, Blomqvist M, Koskinen S, Tupola S, Valkarna E, Nikkola E, et al. Child physical abuse: changes over ten years in the perceptions of Finnish dental professionals. Acta Odontol Scand. 2024;83:433–440. https://doi.org/10.2340/aos.v83.41058.
Mele F, Introna F, Santoro V. Child abuse and neglect: oral and dental signs and the role of the dentist. J Forensic Odontostomatol. 2023;41(2):21–29.
Goulart DR, Colomboi LdA, de Moraes M, Asprino L. What is expected from a facial trauma caused by violence? J Oral Maxillofac Res. 2014;5(4):e4. https://doi.org/10.5037/jomr.2014.5404.
Kvist T, Annerbäck EM, Dahllöf G. Oral health in children investigated by Social services on suspicion of child abuse and neglect. Child Abuse Negl. 2018;76:515–523. https://doi.org.10.1016/j.chiabu.2017.11.017.
Kvist T, Cocozza M, Annerbäck E-M, Dahllöf G. Child maltreatment – prevalence and characteristics of mandatory reports from dental professionals to the social services. Int J Paediatr Dent. 2017;27(1):3–10. https://doi.org/10.1111/ipd.12230.
Kvist T. A dental perspective on child maltreatment. Stockholm: Department of Dental Medicine, Karolinska Institutet; 2016.
Scorca A, Santoro V, Donno AD, Grattagliano I, Tafuri S, Introna F. Early childhood caries (ECC) and neglect in child care: analysis of an Italian sample. Clin Ter. 2013;164(5):e365-71. https://doi.org/10.7417/CT.2013.1614.
Aardal V, Willumsen T, Evensen KB. Differences in anxiety, depression, and oral health-related quality of life among dental anxiety patients with and without reported abuse experience. Eur J Oral Sci. 2024;132(2):e12976. https://doi.org/10.1111/eos.12976.
Levin L, Bhatti C. The role of dental professionals in identifying, reporting, and supporting domestic violence victims. Dent Traumatol. 2024;40(Suppl 2):3–9. https://doi.org/10.1111/edt.1289.
Parish CL, Pereyra MR, Abel SN, Siegel K, Pollack HA, Metsch LR. Intimate partner violence screening in the dental setting: Results of a nationally representative survey. J Am Dent Assoc. 2018;149(2):112–121. https://doi.org/10.1016/j.adaj.2017.09.003.
Maimon-Blau I. Medicolegal aspects of domestic violence against children. Dent Traumatol. 2024;40(Suppl 2):18–22. https://doi.org/10.1111/edt.12899.
Lincoln HS, Lincoln MJ. Role of the odontologist in the investigation of domestic violence, neglect of the vulnerable, and institutional violence and torture. Forensic Sci Int. 2010;201(1–3):68–73. https://doi.org/10.1016/j.forsciint.2010.03.027
Rønneberg A, Nordgarden H, Skaare AB, Willumsen T. Barriers and factors influencing communication between dental professionals and Child Welfare Services in their everyday work. Int J Paediatr Dent. 2019;29(6):684–691. https://doi.org/10.1111/ipd.12507.
Uldum B, Christensen HN, Welbury R, Haubek D. How Danish dentists and dental hygienists handle their role in child abuse and neglect matters. Acta Odontol Scand. 2017;75(5):332–337. https://doi.org/10.1080/00016357.2017.1307448.
Corbei A, Erdal S, Hill N. Samverkan mellan socialtjänsten och tandvården i arbetet med våldsutsatta barn. Soc Med Tidskr. 2024;101(2):188–197.
Sveinsdottir E. Child protection and dental services – children in need are of dentists' concern. Icel Dent J. 2021;1(39):33–9.
Rosen TM, LoFaso VM, Bloemen EM, Clark S, McCarthy TJ, Reisig C, et al. Identifying injury patterns associated with physical elder abuse: Analysis of legally adjudicated cases. Ann Emerg Med. 2020;76(3):266–276. https://doi.org/10.1016/j.annemergmed.2020.03.020.
D'Avolio DA. System issues: Challenges to intimate partner violence screening and intervention. Clin Nurs Res. 2011;20(1):64–80. https://doi.org/10.1177/1054773810387923.
Sprague S, Madden K, Simunovic N, Godin K, Pham NK, Bhandari M, et al. Barriers to screening for intimate partner violence. Women Health. 2012;52(6):587–605. https://doi.org/10.1080/03630242.2012.690840.
Åstrøm AN, Berge KG, Brattabø IV. Reporting suspicion of child maltreatment – a 5-year follow-up of public dental health care workers in Norway. Acta Odontol Scand. 2022;80(3):169–176. https://doi.org/10.1080/00016357.2021.1974936.
Kvist T, Malmberg F, Boovist A-K, Larheden H, Dahllöf G. Clinical routines and management of suspected child abuse or neglect in public dental service in Sweden. Swed Dent J. 2012;36(1):15–24.
Corresponding author: Anna Jinghede Sundwall.
E-mail: anna.jinghede@polisen.se / anna.jinghede@ki.se
The article is peer reviewed.
The article is cited as: Sundwall AJ, Bindslev DA, Rønneberg A, Sveinsdóttir EG, Kvist T, Pyysalo M. The role of the dental team in domestic abuse cases. Nor Tannlegeforen Tid. 2026;. doi:10.56373/697a117e9b767
Keywords: domestic violence, child abuse and neglect, dental neglect, forensic odontology
Akseptert for publisering 24.04.2025. Artikkelen er fagfellevurdert.
Artikkelen siteres som:
Sundwall AJ, Bindslev DA, Rønneberg A, Sveinsdóttir EG, Kvist T, Pyysalo M. The role of the dental team in domestic abuse cases. Nor Tannlegeforen Tid. 2026;136:146-52. doi:10.56373/697a117e9b767